
Vlog, Blogs & More
Vlogs
Blogs
Hip Bursitis vs. Sciatica: How to Tell the Difference and Finally Fix Your Hip Pain
If you have a throbbing, aching pain on the outside of your hip — maybe radiating down your leg — you've probably Googled sciatica. You might have even been told that's exactly what you have. But here's what most people (and many practitioners) miss: hip bursitis is one of the most common causes of hip pain and is one of the most frequently misdiagnosed conditions because it can mimic sciatica almost perfectly.
Before you resign yourself to another round of injections, another MRI, or another provider that sends you home with the same exercises that haven't worked — read this first. We're going to cover exactly what hip bursitis is, how to test yourself at home to confirm the diagnosis, and the short-term and long-term strategies that actually fix the root cause.
What Is Hip Bursitis (and What Is a Bursa, Exactly)?
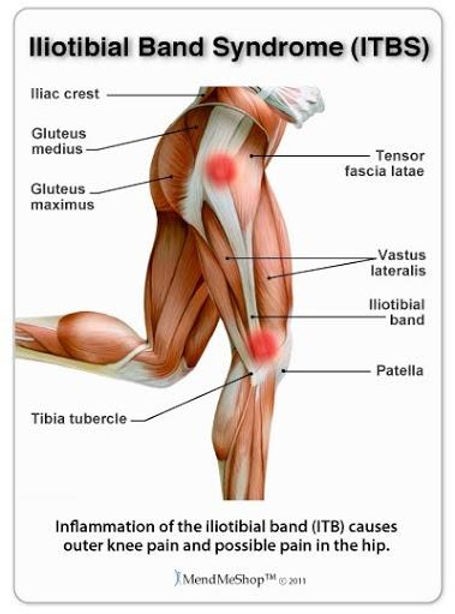
A bursa is a fluid-filled sac that sits between tendons and bony surfaces to reduce friction during movement. At the hip, the bursa — called the trochanteric bursa — sits over the greater trochanter, the bony prominence you can feel on the outer side of your hip.
Here's why this matters: six muscles attach directly to that greater trochanter. Every time you walk, climb stairs, or stand on one leg, those tendons glide across the bursa. When your movement patterns are off — even slightly — those tendons create excess friction and tension on that bursa. Over time, it becomes inflamed, irritated, and painful.
That condition is greater trochanteric bursitis, commonly called hip bursitis.
What makes it especially tricky is that the pain pattern — outer hip pain that radiates down the leg — can look identical to sciatica or even piriformis syndrome. That's why proper assessment is step one before you ever touch an exercise.
Hip Bursitis vs. Sciatica: Why It Gets Misdiagnosed So Often
Sciatica is nerve pain originating from the lumbar spine. Hip bursitis is soft tissue inflammation at the outer hip. They feel similar because the pain pathway overlaps — both can refer pain down the lateral leg.
The critical difference is the root cause and the location of the primary irritation:
Sciatica: Pain originates from nerve compression in the lower back or deep glute (piriformis)
Hip Bursitis: Pain originates from the trochanteric bursa on the outer hip
IT Band Syndrome: Often co-occurs with hip bursitis; pain runs down the outside of the thigh to the knee
SI Joint Dysfunction: Pain is localized between the sacrum (tailbone) and ilium (pelvic bone)
Getting this wrong means doing the wrong exercises — which can make both conditions worse. That's why the tests below are non-negotiable.
How to Test Yourself for Hip Bursitis: 5 Diagnostic Tests
The goal here is to collect multiple "yes" answers. Two or three positives across these tests is strong confirmation that hip bursitis — not sciatica — is what you're dealing with.
1. Posture Test
Stand naturally, the way you would in a grocery store checkout line. Notice which hip you're leaning on.
Most people with hip bursitis unconsciously shift their weight onto the aggravated hip, locking that knee out and dropping into the joint. When you lock your knee and shift to that side, your pelvis shifts and you shut off your glute muscles entirely — creating passive, unrelenting tension on the bursa without any muscular support.
Positive sign: You default to standing on your affected leg with a locked knee.
Quick fix: Unlock the knee, distribute weight evenly on both legs. Shift your weight back into your hips and heels lightly. This should feel unnatural but better.
2. Single-Leg Balance Test
Anyone who walks without a cane or hiking pole should be able to balance on one leg for 30 seconds. While you hold that balance, watch your hips in a mirror:
Are your shoulders and hips level?
Or does one hip drop, or does your trunk shift to the side to compensate?
Are you able to maintain balance for 30 seconds without stepping or touching the counter?
A hip drop during single-leg stance is a classic sign of glute medius weakness — one of the primary muscle imbalances driving hip bursitis.
Positive sign: You cannot balance 30 seconds, or your hip drops/trunk shifts during the attempt.
3. Tenderness-to-Touch Test
Find your greater trochanter — the bony point on the outer side of your hip. Now trace a semicircle around it. Press gently at three points: slightly above, directly on, and slightly below that prominence.
Is it tender? Note exactly where. This maps which muscles and tendons are most irritated, and it tells us which exercises to prioritize.
Bonus: While you're here, move two to three inches toward your front pocket and press into the TFL (tensor fasciae latae) — right at the front-outside of the hip. Then follow that tissue down the outer thigh to the outside of the knee and press two to three inches above it. Tenderness at either of these points suggests IT band syndrome is also in the picture.
Positive sign: Tenderness at or around the greater trochanter, TFL, or outer knee.
4. FABER's Test
Lie on your back. Place your affected leg in a figure-4 position — ankle resting just above the opposite knee. Gently press down on the crossed knee and hold.
Notice where you feel it:
Front of the hip: Hip flexor tension or hip joint involvement
Outer hip (your bursitis spot): Confirms trochanteric bursa irritation
Lower back: Suggests lumbar involvement — potentially sciatica
Positive sign: Pain or pressure at your outer hip (the bursa area).
Also use this position to assess hip rotation. From FABER's, you should have roughly 20–30° of external rotation and 30–40° of internal rotation. Restriction in either direction points to muscle tightness that's loading the bursa.
5. Hip Range of Motion Test (Side-Lying)
Lie on your unaffected side. Keeping your pelvis still (place a hand on it to monitor), lift your top knee — how high can it go? Then, with the knee bent, extend the leg backward — how far?
Normal ranges: approximately 120° of hip flexion and 10–20° of hip extension.
Loss of hip extension is particularly important. Limited extension forces your body to compensate with lumbar movement and puts relentless load on the outer hip structures. If you also feel a pinch in the front of the hip during this test, note that — it's outside the scope of hip bursitis and warrants separate evaluation.
Positive sign: Restricted range of motion, especially into extension, with or without reproduction of your familiar hip pain.
Short-Term Hip Bursitis Pain Relief
Before we fix the root cause, let's take the edge off. These strategies are about creating enough relief to let you move and do the real work.
KT Tape / Rock Tape
Kinesiology tape applied over the trochanteric bursa and fanning across the glutes (mimicking the pull of the muscles themselves) provides meaningful short-term pain relief for many people with hip bursitis. Use one 4-inch anchor strip directly over the bursa and three 6–8 inch strips fanning outward, applied with 20–25% stretch on the working strips and no tension on the anchors.
Clean the skin first with rubbing alcohol or hand sanitizer. Anchor on skin when possible.
This is a band-aid — not a fix — but it buys you enough comfort to train properly.
Piriformis / Glute Stretch
Lying on your back, cross your affected leg over and pull it toward the opposite shoulder. Keep your pelvis flat — we don't want your lower back rocking. This stretches the external rotators and posterior glute fibers.
Hold 20–30 seconds, breathe through the stretch, and back off if you feel any sharp pain. You should feel a gentle pull through the glute — not a pinch.
Thomas Stretch (Hip Flexor / Quad)
Sit on the edge of your bed or couch and lean back. Let your affected leg drop off the edge toward the floor. The goal is to lower the heel while keeping your lower back neutral (no arching). Engage your glute and actively drive that hip into extension.
This stretch directly addresses the hip flexor tightness that typically accompanies hip bursitis — especially when IT band syndrome is also present.
Foam Rolling: Glutes, TFL, and Quads
Use a three-point support system (two arms and one leg, or two hands and one knee on the floor) to offload some of your bodyweight while you work.
Glutes: Work at a 45° angle across the muscle. Find hot spots and spend 30–60 seconds working through them with slow, controlled pressure.
TFL: Roll along the front-outside of the hip. Once you find the hot spot, add movement — bring your bottom leg forward and back (into hip flexion and extension) to create an active release while the roller pins the tissue.
Outer Quad/IT Band: If the lateral thigh is numb or hypersensitive, use the side of your forearm instead of the roller to gently mobilize the tissue.
One minute per area is enough. When you stand up and feel noticeably looser — that's the confirmation that tissue restriction was part of your pain picture.
Long-Term Hip Bursitis Treatment: Fix the Root Cause
Short-term relief is step one. But if you stop there, the pain will come back — usually within a few weeks. That's the cycle most hip bursitis sufferers are stuck in.
The reason hip bursitis keeps returning is almost always the same: motor control imbalances, muscle weakness, and compensatory movement patterns that never got corrected. Specifically:
Glute medius weakness → hip drop during walking and single-leg stance
Glute maximus weakness → poor hip extension mechanics
VMO (inner quad) weakness → unstable knee alignment during movement
Poor hip rotation control → excess stress on the bursa with every step
Here are the exercises that address all of it:
Single-Leg Heel Touch / Step-Down
Stand on a step with your affected leg. Lift the opposite leg slightly forward. Then hinge at the hip — sit back into your hip and heel — lowering until your non-affected heel lightly taps the floor below the step. Drive back up, squeezing your glute and inner quad (VMO) at the top.
This is a demanding exercise. Start with 2 sets of 8–12 at about 60–70% of your maximum depth, always pain-free. Progress depth over weeks, not days.
Focus on keeping your hips and shoulders level throughout. No trunk shifting. No hip dropping.
Hip Airplane (Hip Hinge with Rotation)
Stand on your affected leg, knee soft. Hinge forward at the hip, keeping your pelvis level, and lift the opposite leg behind you. From this position, drop the free hip toward the floor (internal rotation stretch) and then rotate it open toward the ceiling (external rotation activation), squeezing through the glute at the top of each rotation.
Fix your gaze on a single point on the wall — vision contributes roughly 60% of your balance, and this is a complex movement. Control is everything here.
This exercise simultaneously stretches and activates the hip stabilizers, making it one of the highest-value movements for hip bursitis recovery.
Programming: 2 sets of 8–12 reps, staying pain-free, 60–70% effort.
The Biggest Mistake People Make with Hip Bursitis
The most common mistake — and the reason so many people end up back in pain within weeks of feeling better — is stopping the work the moment symptoms improve.
Hip bursitis pain decreases before the underlying movement dysfunction is corrected. When the pain fades, the temptation is to return to normal activity without maintaining the strengthening and movement work. Within a few weeks, the compensation patterns reload the bursa, and the cycle starts again.
The fix is simple but it requires discipline: test and retest. Can you now pass the single-leg balance test? Is your hip ROM restored? Can you complete the step-down exercise with level hips and no pain? Those benchmarks — not absence of pain — are the real indicators that you're ready to reduce the intensity of your rehab.
Ready to See Every Step in Action?
Reading about diagnostic tests and exercises is useful — but watching them performed correctly is what actually lets you replicate them. Dr. Nick walks through every single test, stretch, taping technique, and exercise in this complete hip bursitis video, including real-time cueing so you know exactly what to feel and look for.
👉 Watch the Full Hip Bursitis Tutorial Here — 18-Min Hip Bursitis Pain Relief Treatment (Complete PT Session)
If you've been bounced between practitioners, told your imaging "looks fine," or had relief that keeps fading, this video gives you a functional movement framework that most providers never apply to hip pain. Watch it, test yourself, and start building toward lasting resolution.
Frequently Asked Questions About Hip Bursitis
How do I know if I have hip bursitis or sciatica? The key distinction is the location of primary tenderness. Hip bursitis produces tenderness directly over the greater trochanter (outer hip bony prominence) and is aggravated by FABER's test and single-leg stance. Sciatica originates in the lower back and is typically aggravated by spinal flexion or nerve tension tests. Both can radiate pain down the leg, which is why hands-on assessment matters.
Can hip bursitis heal on its own? It can improve temporarily, but without correcting the movement patterns and muscle imbalances that caused it, it almost always returns. Lasting resolution requires addressing glute medius strength, hip rotation control, and postural habits.
What makes hip bursitis worse? Standing with a locked knee on the affected side, prolonged sitting with legs crossed, sleeping on the affected side without a pillow between the knees, and walking with a hip drop. All of these increase tension on the bursa.
How long does hip bursitis take to heal? With consistent, correctly targeted exercise, most people notice significant improvement within 4–8 weeks. Full functional recovery — where the compensation patterns are corrected — typically takes 8–16 weeks depending on severity and how consistently the program is followed.
Is it safe to exercise with hip bursitis? Yes, with the right exercises at the right intensity. The guiding principle is no pain, all gain — stay at 60–70% of your maximum capacity and keep all movement pain-free. Exercises that reproduce sharp pain at the bursa should be modified or regressed.
Should I use ice or heat for hip bursitis? In the acute phase (flare-up with swelling or significant tenderness), ice for 10–15 minutes can help reduce inflammation. For chronic hip bursitis, heat or contrast therapy may be more helpful before exercise to improve tissue mobility.
Dr. Nick is a Doctor of Physical Therapy and Functional Movement Therapist. The FMT 360 Method is his system for identifying and resolving the root causes of musculoskeletal pain — not just managing symptoms.
For a full guide to evaluating your hip and back pain from home visit: https://www.functionalmovementtherapy.com/guide-to-a-better-diagnosis

Reels
Download your FREE "Guide To A Better Diagnosis" today!
This self-examination guide will help you to both diagnose your pain & categorize your symptoms, more than most specialists will do an in appointment you'll wait months for.
Unlock Your Potential with One Click
Experience the FMT 360 Revolution Today!

.
Links
Contact
8:00am – 5:00pm Monday - Friday (EST)
Closed Saturday - Sunday
Get expert advice for a pain-free back.
Copyright © 2026 Functional Movement Physical Therapy, PLLC, All rights reserved
Copyright © 2023 Functional Movement Physical Therapy, PLLC, All rights reserved